(SSF; also referred to as sacrospinous ligament fixation) is the most commonly studied transvaginal procedure for treating vaginal vault prolapse.
Although SSLS may also improve anterior vaginal wall prolapse, it is less effective for this indication. Thus, women with large anterior wall defects in addition to apical defects may benefit from another type of prolapse repair, which better supports the anterior vagina or concomitant anterior colporrhaphy.
Procedure:
The surgery is performed under general anaesthetic.
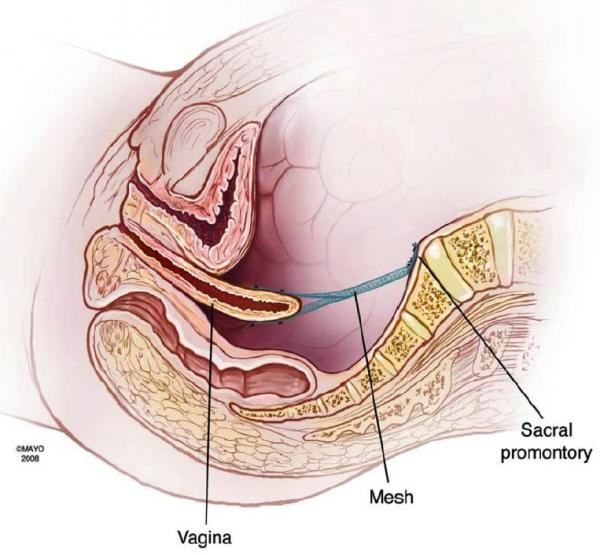
The surgical principal is that the vaginal top is suspended through suturing into the sacrospinous ligament (A ligament in the pelvis).
Before starting the procedure, the patient is examined to ensure that the vagina is long enough to reach the sacrospinous ligament. Women with short Vagina may not be suited for such procedure and an abdominal approach may be more successful.
The procedure is performed vaginally. It can be done in conjunction with other vaginal wall repair procedures and/or incontinence procedures.
The Sutures used are delayed absorbable sutures.
The procedure is usually covered with antibiotics and blood thinning medications to prevent blood clots forming in legs or lungs then after.
See diagram below showing the principals in performing the procedure.
In a literature review of studies, cure rates of prolapse-related symptoms ranged from 70 to 98%.
Recurrence of apical (top of vagina) prolapse after SSLS has been reported in 2 to 19% of women and of anterior vaginal wall prolapse in 6 to 29%. Therefore, as noted above, women with large anterior wall defects in addition to apical descent may benefit from an additional type of prolapse repair, which more directly addresses support of the anterior vagina.
Complications:
Serious complications are uncommon following SSLS.
Some of the complications are: pain, infection, perforation of the rectum or bladder, and pain with intercourse.
Recurrence of symptoms and/or prolapse may occur. Usually this is in another site of the vagina, due to further weakness in the area.
Infectious complications are the most common type of adverse event, and are generally mild (e.g, cystitis).
Buttock pain may occur in up to 15% of cases. Mainly corresponds to the site of the suture. In majority of cases the pain will disappear after a median period laps post surgery.
Recovery Time:
Most women stay in hospital for 2-3 days. You will be sent home once you are feeling well and once you are able to pass urine with no problem.
It is important to rest after the operation and allow the area to heal.
Generally it is recommended that:
You restrict activity for 4 weeks.
After 4weeks do light activities only.
Avoid heavy lifting for 6 weeks, including shopping bags, washing baskets and children.
Abstain from sexual activity for 6 weeks.
Avoid playing sport for 6 weeks.